Endometriosis is primarily thought to be a gynecologic disease that affects the pelvic organs, but it can also exist in the urinary tract. Endometriosis is usually in the pelvis and can lie near the ureter, which may lead to kidney issues such as asymptomatic hydronephrosis or, in rare cases, silent kidney failure.
As such, knowledge of how to read a kidney ultrasound is essential when sonographically evaluating a patient with possible or confirmed endometriosis.
Understanding How Endometriosis Enters the Ureters and Affects the Kidneys
Endometriosis represents an abnormal growth of cells similar to those in the endometrium. However, the growth occurs outside of the endometrium. These cellular deposits have the ability to grow in size, especially in an area of the pelvis called the posterior compartment.
The posterior compartment contains the uterosacral ligaments. They are the most common site for deep endometriosis, which deeply invades the tissue in which it is implanted. The uterosacral ligaments provide a direct connection to the parametrium, the area beside the uterus where the ureters traverse. When endometriosis invades the parametrium, it is very likely that the ureter will be significantly affected (extrinsic ureteral endometriosis) in the form of narrowing, kinking or both. Depending on the severity, hydroureter and hydronephrosis can develop.
In rare cases, endometriosis may initiate in the ureter itself (intrinsic ureteral endometriosis), which yields proximal hydroureter and hydronephrosis. In these scenarios, urgent surgery is necessary to excise endometriosis and decompression of the built-up fluid in the ureter and kidney.
Identifying Endometriosis in the Bladder and Beyond
Although many patients with endometriosis experience pelvic pain, symptoms do not always clearly indicate whether the ureter or kidneys are affected. Performing an ultrasound for endometriosis in a systematic fashion helps clinicians avoid subjective decisions about whether to evaluate the ureters or kidneys. In fact, the urinary tract as a whole is worth evaluating, as bladder endometriosis may also be present.
If bladder endometriosis exists in the trigone or is large enough to compress the ureter openings into the bladder, this may be a source of hydroureter and hydronephrosis. The bladder and ureters can be assessed via transvaginal ultrasound. If this is not possible, then transrectal ultrasound is also an option for assessment. A kidney ultrasound is performed transabdominally. The proximal ureters can be evaluated transabdominally as well; this will not likely identify the source of the obstruction, though, which is very distal along the course of the ureter as it traverses the parametrium.
Adopting Best Practices for Bladder and Ureter Ultrasound
In the case of transvaginal ultrasound for endometriosis, it is best if the patient empties their bladder prior to the scan. If a physician leaves the bladder evaluation until near the end of the scan, a small amount of urine has usually collected; this is ideal, as the urine slightly separates the bladder walls, permitting better evaluation of the various bladder layers, including the mucosa and the muscularis propria.
The muscularis of the bladder wall is the layer most likely to be affected by deep endometriosis, while the bladder base and dome are the most likely sites of deep endometriosis. Endometriosis may appear as hypoechoic linear or spherical lesions with or without regular contours.
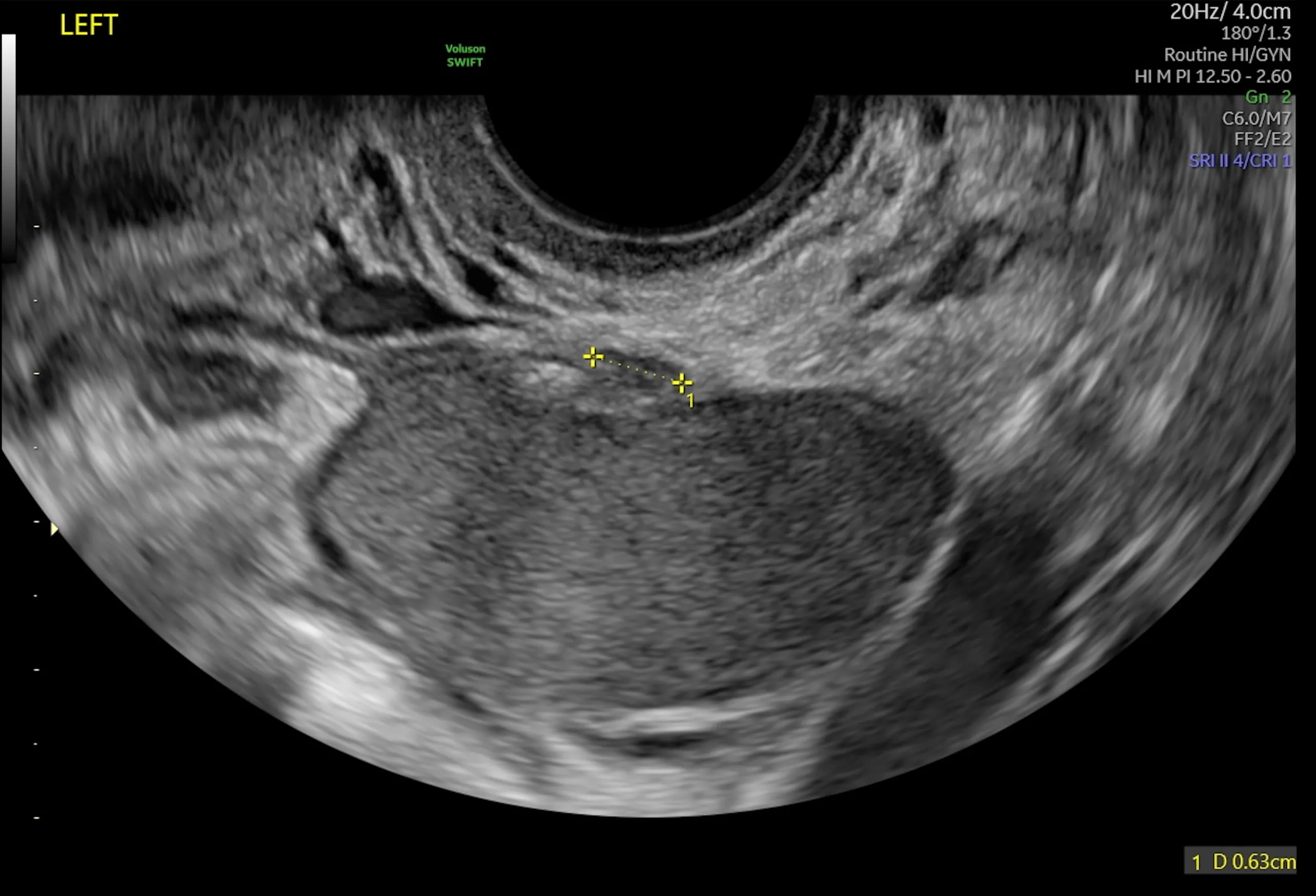
After a thorough evaluation of the bladder, the ureters should be evaluated. Research published in Ultrasound in Obstetrics and Gynecology describes in great detail how to visualize the ureters on ultrasound. The operator should hold the probe midline in the sagittal plane, pointing toward the bladder. A slightly compressed bladder that is mostly out of view, with only the bladder base remaining partly in view, is the ideal starting point for ureter visualization.
Once in this position, move the probe laterally toward the pelvic wall, remaining in that same horizontal plane. In normal cases, the ureter will appear as a hypoechoic tubular structure, which will contract to move urine from the kidneys to the bladder. Follow the ureter as proximally as possible, at least to the level that the ureter crosses the uterine vessels. Since ureteral endometriosis often occurs in the parametrium, evaluation of only the distal ureter is insufficient to identify areas of obstruction and proximal dilation such as hydroureter. Watching for vermiculation allows the sonographer to better identify areas of obstruction.
Assess both ureters to ensure symmetry is present. Asymmetry may signal an abnormality, which can include ureteral endometriosis but may also depict non-endometriosis pathology. If there is a concern for hydroureter, the largest diameter of the ureter during maximum dilation should be measured. Though evidence is scarce on what measurement defines hydroureter, separate research published in Ultrasound in Obstetrics and Gynecology describes a ureter diameter of greater than 6 mm in all cases of ureteral dilation visualized surgically.
When hydroureter is identified, the distance between the site of obstruction and the distal ureteral orifice (where the ureter enters the bladder) should be measured to help with surgical planning. When surgery is planned to excise ureteral endometriosis, factors such as identifying the location of the endometriosis on the ureter and/or where the ureter is being compressed can dictate the specific type of surgery needed.
Performing an Ultrasound of the Kidney
Clinicians are advised to perform a transabdominal kidney ultrasound routinely in all patients with confirmed or suspected endometriosis. The potential consequences of missing hydronephrosis due to endometriosis, including silent kidney failure, are significant. The ability to recognize uterosacral ligament or parametrial endometriosis, which affect a ureter to cause hydronephrosis, is still a developing skill set. According to a pictorial guide from the Australasian Journal of Ultrasound in Medicine, transvaginal ultrasound assessment of hydroureter alone may not alert physicians to evaluate the kidneys.
Learning how to read a kidney ultrasound for hydronephrosis due to endometriosis is relatively simple. A study published in BJU International showed that interobserver agreement was excellent for the grade assessment of hydronephrosis using ultrasound. A kidney ultrasound can also be performed quickly without dramatically extending the length of a patient visit.
In an adult patient, a curved array transducer should be used, suggests a pictorial review published in Diagnostics. The entire kidney can be assessed during either normal breathing or while the patient holds their breath to help avoid artifacts created by the lower ribs. Supine position can be attempted, but the kidneys may be obscured by bowel gas. The lateral decubitus positions (right and left) mark one alternative for assessing the kidneys. Regardless, the evaluation should be initiated in the longitudinal scan plane, parallel to the long diameter of the kidney. The kidney is easier to distinguish with this orientation.
With hydronephrosis, an elongated, fluid-filled (anechoic) space is seen in the central portion of the kidney. Normally, the dilated pelvis can be differentiated from the dilated calyces. If hydronephrosis is identified, the severity of the hydronephrosis should also be classified.
Ultrasound evaluation of the urinary tract system — especially the bladder, ureters and kidneys — is essential when assessing someone with suspected or confirmed endometriosis. Performing a combination of transvaginal and transabdominal ultrasound techniques may help patients prevent unnecessarily losing a kidney to endometriosis.